Nanjing Elephant-Med instrument Co. , Ltd.
MOBILE:
ADDR:86 Shuanggao Road, Economic Development Zone, Gaochun District, Nanjing City
WEBSITE:http://www.elephant-med.com/




ligasure, bipolar, surgical electrode, high frequency surgical system
POSITION: HOME > EN > Product articles
ABOUTUS
PRODUCTS
roduct categoryCONTACT
ontact usNanjing Elephant-Med instrument Co. , Ltd.
MOBILE:
ADDR:86 Shuanggao Road, Economic Development Zone, Gaochun District, Nanjing City
WEBSITE:http://www.elephant-med.com/
Electrosurgery is a term used to describe the various ways in which electrical energy is used to cause thermal destruction of tissues through dehydration, condensation, or vaporization. The two most commonly used electrosurgical techniques are high-frequency electrosurgery and electrocautery.
Electrosurgery is not synonymous with electrocautery, but it is often incorrectly referred to as electrocautery in practice and in the literature.
High-frequency electrosurgery involves four different methods: electrocoagulation, electrodesiccation, electrofulguration, and electrosection. It uses high-frequency alternating current to convert electrical energy into heat energy due to resistance, and heat energy accumulates in the tissue to achieve different degrees of tissue thermal damage. This method is often used for extensive hemostasis and exfoliation surgeries.
Electrocautery, also known as cautery.It refers to the direct current or alternating current that generates heat through a resistive wire electrode (hand-held element), and the heated hand-held element is applied to living tissues to achieve hemostasis and varying degrees of tissue destruction. It is commonly used in a variety of minor surgical procedures in ophthalmology, dermatology, otolaryngology, plastic surgery, and urology. In this method, the current is not passed through the patient, so the procedure is safe for patients with electronic implants that remain functional in the wet field.
Many refer to Bovie as the "father of electrosurgery".
But before Bovie, the physics behind these instruments were known. As early as the early 20s of the 20th century, surgeons used cautery and electrical energy in medicine. At that time, Bovie developed modern instruments and brought them to the forefront of the industry. Nowadays, more and more electrosurgical devices are used in the operating room, but ablation is undoubtedly the most commonly used technique.
Cautery dates back to prehistoric times, when heated stones were used to achieve hemostasis. As early as the 6th century B.C., conduction heating of tissues was already a well-known medical tool.
The use of electrical energy in medicine coincides with the discovery of electricity in the 18th century.
Three Epochs in the Development of Electrosurgery:
The first era began with the discovery and use of static electricity, and the time frame of this era is not known.
The second era, also known as the electroplating age, evolved from Luigi Galvani's accidental discovery in 1786. (He pointed out that painting the iron railing at home induced muscle spasms in the frog's legs hanging from the copper structure) His discovery and subsequent experiments gave birth to electrophysiology.
In 1831, the discoveries of Faraday and Henry ushered in the third era. Almost simultaneously, they showed that a moving magnet could induce an electric current in the wire.
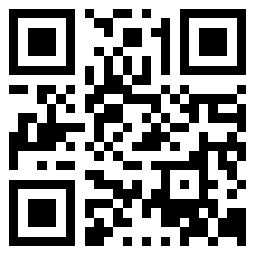
In 1881, Morton discovered that oscillating currents with a frequency of 100kHz could pass through the body without causing pain, spasms, or burns.
Around the beginning of the 19th century, people began to become aware of the medical uses of electricity. In 1897, Franz discovered that patients with diseases of the joints and circulatory system could benefit from the use of electric currents. He used the term "diathermy" to describe this thermal effect.
In 1900, Joseph, a Parisian physician, used a similar generator to electrotherapy an insomniac patient when he noticed that sparks from the electrodes condensed an area of his skin. He then used this arc current to treat a cancerous ulcer on a patient's hand. This event is believed to be the first time that an electric current was actually used in a surgical procedure. Over the next decade, the use of electric currents to treat lesions of the skin, mouth, bladder, as well as for clotting and hemostasis of vascular tumors became commonplace.
At the beginning of the 20th century, Simon Pozzi used high-frequency, high-voltage, low-ampere currents to treat skin cancer, a technique he called "fulguration". Later Doyen made improvements by attaching a grounding pad to the generator and placing it underneath the patient. He found that this helped the electric current penetrate deeper into the tissue and had an "electrocoagulation" effect.
Around 1910, William Clark improved the instrument so that the current increased and the voltage decreased, resulting in a hotter and shorter electrical spark that penetrated deeper into the tissue. In addition, he replaced a single spark with a multi-spark system that produced a smoother current. Under the microscope, he found that the tissues were dehydrated and atrophied under the influence of electric current. In 1914, he used the term "desiccation" to describe the effect of tissue destruction and carbonization caused by dehydration. He became the first American to routinely use this method to remove malignant growths on the skin, head and neck, breasts, and cervix. Clark's transformation laid the groundwork for Bovie and Cushing's later research.
Boive, building on the findings of previous researchers, built the electrosurgical unit to create an electrosurgical generator that can generate high-frequency currents, which are transmitted by a "cutting loop" for cutting, coagulation, dehydration and drying. On October 1, 1926, Dr. Cushing of Brigham Hospital in Boston used his instruments for the first time in the operating room to remove an enlarged vascular myeloma from the head of a 64-year-old patient.
Prior to 1970, electrosurgical generators were "ground referenced", and the flow of energy was connected in parallel with the earth. In this case, whenever the patient comes into contact with a potential ground path, the current chooses the path of least resistance, which may result in the current passing through the ECG monitoring electrodes or the IV pole in contact with the patient. If the density of the current through the contact is high enough, there is a risk of burns to the patient.
By using a generator isolated from the ground, the current is confined between the acting electrode and the patient loop electrode (a dispersion pad placed on the patient), thus providing a low-resistance path for the current to return from the patient to the generator, reducing the potential hazards.
High Frequency Electrosurgery:
High-frequency electrosurgical techniques essentially provide two types of energy delivery devices: unipolar and bipolar. Among them, the "Bovie" electric knife is the most representative.
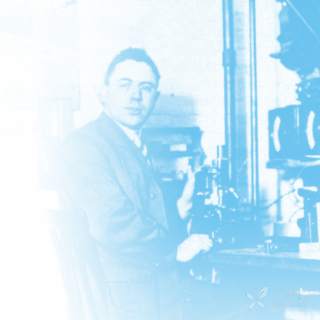
Unipolar device: The monopolar electrosurgical unit transfers energy to the tissue, requiring an electric current from the generator to pass through the patient's body from the acting electrode and exit through a dispersion pad connected to the generator to form a complete circuit.
Bipolar device: The bipolar electrosurgical unit does not require a dispersion pad, and the functions of the acting electrode and the loop electrode are completed in the surgical part. The current does not pass through the patient but is confined to the tissue between the forceps, and when the target tissue is clamped, the complete circuit can be completed.
Unipolar devices are at the highest risk because they need to pass an electric current through the patient's body, causing electromagnetic interference to implantable electronic devices.
Bipolar devices are a safer form of electrosurgery, where the current is confined to the target tissue, thereby minimizing the random dispersion of electrons in the body and interaction with the implanted electronic device. When used properly, the data suggest that bipolar electrosurgery poses no risk of cardiac device failure.
A high-frequency electrosurgical unit typically consists of a generator and a handpiece with multiple electrodes. The device is controlled by a switch or footswitch on the nose.
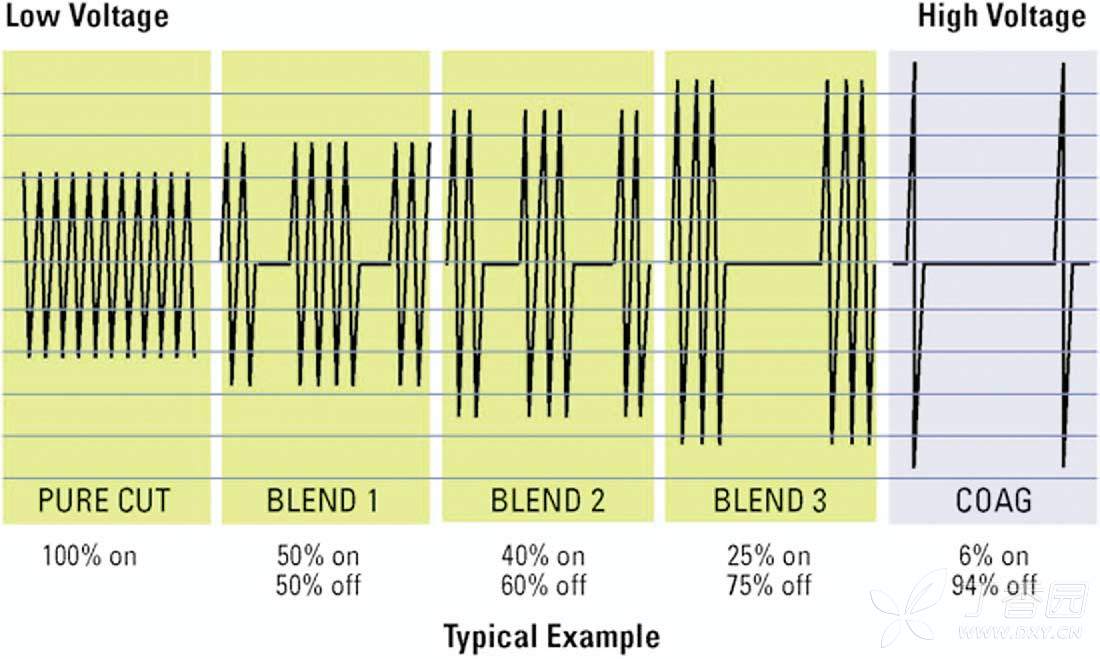
The current output from the generator can be modulated to deliver different waveforms to the tissue, and when the output waveform changes, the corresponding tissue effect will also change.
In cleavage mode, due to its continuous current delivery, high tissue temperatures are generated in a short period of time, resulting in rapid expansion and explosive vaporization of cell contents.
In condensation mode, the intermittent transfer of current results in less heat generation, forming a clot as the tissue slowly rises.
In addition to pure cutting and clotting modes, there are also hybrid modes, i.e., adjusting the degree of intermittent (duty cycle) to achieve different levels of cutting and clotting.
Electrocautery:
Electrocautery is a way of transferring heat directly to the tissue, using a low-voltage, high-ampere current to heat the hand-held element before acting on the tissue instead of passing the current through the tissue, so it is generally considered the safest electrosurgical look.When the use of high-frequency electrosurgical instruments is prohibited, electrocautery is the most commonly used method.
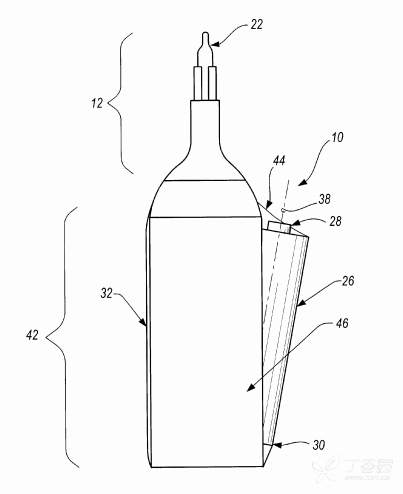
In the medical field, it is well known to use instruments to cauterize the patient's tissue to close ruptured blood vessels and close wounds. Typically, this cautery device is a battery-powered, hand-held device that includes a cautery element, a heating unit, a switch assembly, and an enclosure. Because of the size and convenience of the cauterizer, its use has expanded to include tasks such as suture removal.
Each electrocautery device transfers heat in a single or a range of temperatures ranging from 200 degrees Celsius to 1200 degrees Celsius, and most devices also include a choice of tips such as ring tips, fine tips, and needle tips.
Hypothermia can be used to treat superficial and relatively avascular lesions of superficial tissue destruction;
Higher temperatures can be used to remove thicker skin lesions.
Safe use and precautions:
There are many indications for electrosurgical techniques, and in many cases, electrosurgical instruments are combined with another modality, such as scalpels, surgical scissors, spatula. There is a conventional dogma in surgery that the skin is opened with a traditional scalpel and then the deeper tissue is opened with an electric knife.
In a monopolar electrosurgical unit, the activating electrodes are placed at the surgical site and the dispersing pads are placed elsewhere on the patient's body. When the current loop is completed, the current needs to pass through the patient's body. The function of the dispersing pad is to safely remove the current from the patient, but over time, burns can occur if the heat generated cannot be safely dissipated through the dispersing pad.
In bipolar electrosurgical equipment, the functions of the activating electrode and the circuit electrode are performed at the re-operation site, and only the tissue caught by the forceps can be passed through the current without the need for a dispersion pad placed on the patient, which greatly reduces the possibility of accidental current dispersion and burns.
In an electrocautery device, an electric current cannot enter the patient's body, but instead flows through a heating element that cauterizes the tissue by transferring heat directly through a heated wire, often like a portable hand-switch, battery-powered device. Depending on the site and type of surgery, the surgeon can choose different temperatures and tip shapes. It is often used for incision and hemostasis in delicate surgical procedures.
Anatomical location and presence of implantable electronic devices are the two main considerations when evaluating contraindications to electrosurgery.
Anatomical sites involved include the area around the eyes and sites with narrow stems or bases such as scrotum, fingers, and large papillary cancers.
Applying an electric current to a narrow stem or base can cause a phenomenon called the "channel effect". That is, when the current passes through, it will concentrate in the narrow area, which will lead to the possibility of tissue damage at the base. If the current is exposed and conducts along tissues that are more conductive than the surrounding tissues, such as nerves and blood vessels, the channel effect may also cause distant injury. This channeling effect, if it appears on the fingers and penis, can lead to distant condensation with serious consequences.
Eye damage is not the result of the groove effect, but rather caused by sparks or direct thermal injury, which can be prevented by avoiding the use of electrodes near the eye or by using corneal shields.
Although not an absolute contraindication to high-frequency electrosurgery, electromagnetic interference from implantable electronic devices (e.g., pacemakers for the heart and stomach, implantable cardioverter-defibrillators, cochlear implants, and deep brain, nerve, and bone marrow stimulators) is a highly discussed risk. Patients using these devices require a thorough preoperative evaluation and may require intraoperative monitoring and postoperative device evaluation.
In electrocautery, an electric current is not passed through the body, so the procedure can be safely used in patients with electronic device implants. In addition, the heat is concentrated at the very fine tip, which greatly reduces thermal damage to the surrounding tissues.
The main risk of electrocautery is that when the instrument is used directly on the tissue above the implant, it may cause thermal damage to the device below.
The physician must consider the histological properties of the tissue being treated, the area and depth of destruction required, possible complications, and the performance of the different devices. The common principle of all electrosurgical procedures is to use as little power as possible to achieve the desired effect, thus limiting damage to adjacent tissues.
The principle of infection transmission also applies to electrosurgery and electrocautery.
There are three potential modes of infection transmission during surgery, including treatment electrodes, surgical smoke, and nebulized blood droplets. Animal skin tests have shown that hepatitis B virus, human papillomavirus, and Staphylococcus aureus can be transmitted through electrodes to uninfected sites.
During electrosurgery, nebulized blood droplets can be pushed up to a distance of 30 cm and can be contagious if inhaled. In addition to dangerous chemicals and carcinogens, surgical smoke can also contain live viruses and bacteria. Smoke from the treatment of warts with high-frequency electrocoagulation has been identified as active HPV.
To prevent the spread of infection, a smoke extraction system should be used, as well as face shields, protective eye shields, and surgical gloves. A sexual or sterilized electrode should be used.
【DOS】
● When not in use, the handheld head should always be placed in a non-conductive case.
●Always use the lowest possible generator equipment to achieve the desired surgical results, when the voltage used is higher than necessary, the possibility of arc formation increases, and if the setting is continued to be turned up, there may be damage to the interface between the skin and the dispersion pad
● Clean the electrode tip frequently, due to the accumulation of coke at the tip, the resistance increases, which can cause the coke to form arcing, sparks, ignition, and combustion. When cleaning the electrodes, the coke should be wiped off with a sponge instead of a regular pad, as these pads will create a groove in the tip of the electrode, increasing the build-up of coke
【DON'TS】
●Electrosurgical instruments should not be used in the presence of flammable agents or oxygen-rich environments
●Avoid flammable substances that can be ignited by sparks, such as alcohol and skin degreasers. If alcohol-based skin preparation materials must be used, make sure that the solution is completely dry and that the smoke has dissipated before activating the device.
●Wires should never be wrapped around metal instruments to prevent current from flowing into metal instruments and causing burns.
●Determine whether the patient has any metal implants, including pacemakers. If the dispersion pad is placed on the skin with a metal implant, it may cause injury
●Place the dispersion pad as close to the surgical site as possible, choosing a clean, dry, well-vascular and large muscle mass. Avoid lone star bulges, adipose tissue, scar tissue, skin with metal implants, hairy surfaces. Make sure that the dispersion pad is evenly distributed with the patient's skin
Related research results sharing:
Research by Kearns and colleagues has shown that electrosurgical incisions are better in laparotomy than scalpel incisions. In this study, patients with a Bovie electrosurgical pen had a similar rate of wound infection on the first and second days after surgery as those with a conventional scalpel, while pain scores were lower.
Pearlman and colleagues have published an article showing that in open cholecystectomy compared to scalpel and laser knife, the use of an electric knife results in a deeper incision, a faster cut, and less blood loss from the incision, with no significant difference in the patient's subjective or objective pain scores.
The Future of Electrosurgery:
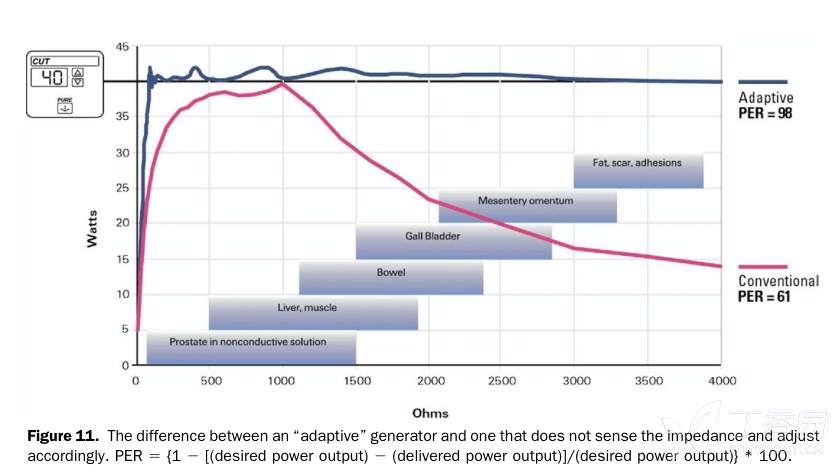
The electrosurgical operating room is a growing field and is actively researching new applications. Today's electrosurgical generators use a closed-loop control loop to regulate voltage and current, and have maintained a constant power output as the activated electrode passes through the tissue of varying resistance. These "adaptive" generators are a big improvement over traditional electrosurgical generators.
Due to the development of technology to incorporate more sophisticated computer-on-chip technology into electrosurgical generators, the potential to increase to clinical applications is developing at an alarming rate, and radiofrequency energy is being widely used in the cautery treatment of many target tissues. From arrhythmias to liver cancer, radiofrequency energy for electrosurgery is seeking new applications.
Based on the experience of vascular occlusion and protein fusion, optimized electrosurgical energy delivery may be successfully used in the future to accomplish lung parenchymal closure, intestinal and vascular anastomosis. This technology also enables skin grafting without the need for a foreign body. In the not-too-distant future, hernia repair can be done by fusing an artificial dermis or similar tissue to the edge of the defect, eliminating the need for prosthetics and the complications they cause.
In conclusion, electrosurgery remains an essential technique that surgeons need to master. At the heart of developing this skill is a comprehensive understanding of the biophysical roles of electrosurgical energy and interstitial tissues. Research in the field of tissue interaction shows the potential for innovative applications in electrosurgery. In addition to improving electrosurgical cutting and hemostasis, tissue fusion and ablation are becoming more and more widely used in surgical procedures. A better understanding of this technology is essential to improve patient outcomes and use it safely.
Reference:
1.Electrosurgery:History,Principles,and Current and Future Uses,Article in Journal of the American College of Surgeons,April 2006
2.Cautery Apparatus And Method,Ronald D.Shippert,4975 S.Albion St.,Littleton,Co(US)80121.
PREV:No more
NEXT:The most frequently used instrument in surgery? Energy Devices
WEB SITE:http://www.elephant-med.com/
TEL:025-57852662
WeChat:ailifen0002 EMAIL:support@elephant-med.com
Nanjing Elephant-Med instrument Co. , Ltd. 86 Shuanggao Road, Economic Development Zone, Gaochun District, Nanjing City ICP No.:苏ICP备2025153396号-1  苏公网安备32011802010375号 互联网药品信息服务资格证书编号:(苏)-非经营性-2024-0128
苏公网安备32011802010375号 互联网药品信息服务资格证书编号:(苏)-非经营性-2024-0128